

WHAT WE KNOW ABOUT HANTAVIRUS RIGHT NOW
A cruise ship. Three dead. Six countries. And a virus most Americans had never heard of until this week.

On May 2nd, the World Health Organization received an alert that stopped global health officials in their tracks. A cluster of passengers aboard a Dutch-flagged cruise ship in the Atlantic Ocean were developing severe respiratory illness. Two of them were already dead. A third was critically ill. The ship, the MV Hondius, was somewhere in the South Atlantic with 147 people still on board and no port willing to take it.
The culprit, confirmed four days later, was hantavirus. Specifically, the Andes virus, a strain normally found in South America and one of the deadliest respiratory viruses known to medicine. And unlike almost every other hantavirus in existence, the Andes virus can spread between people.
That last sentence is the one that matters.
What hantavirus actually is
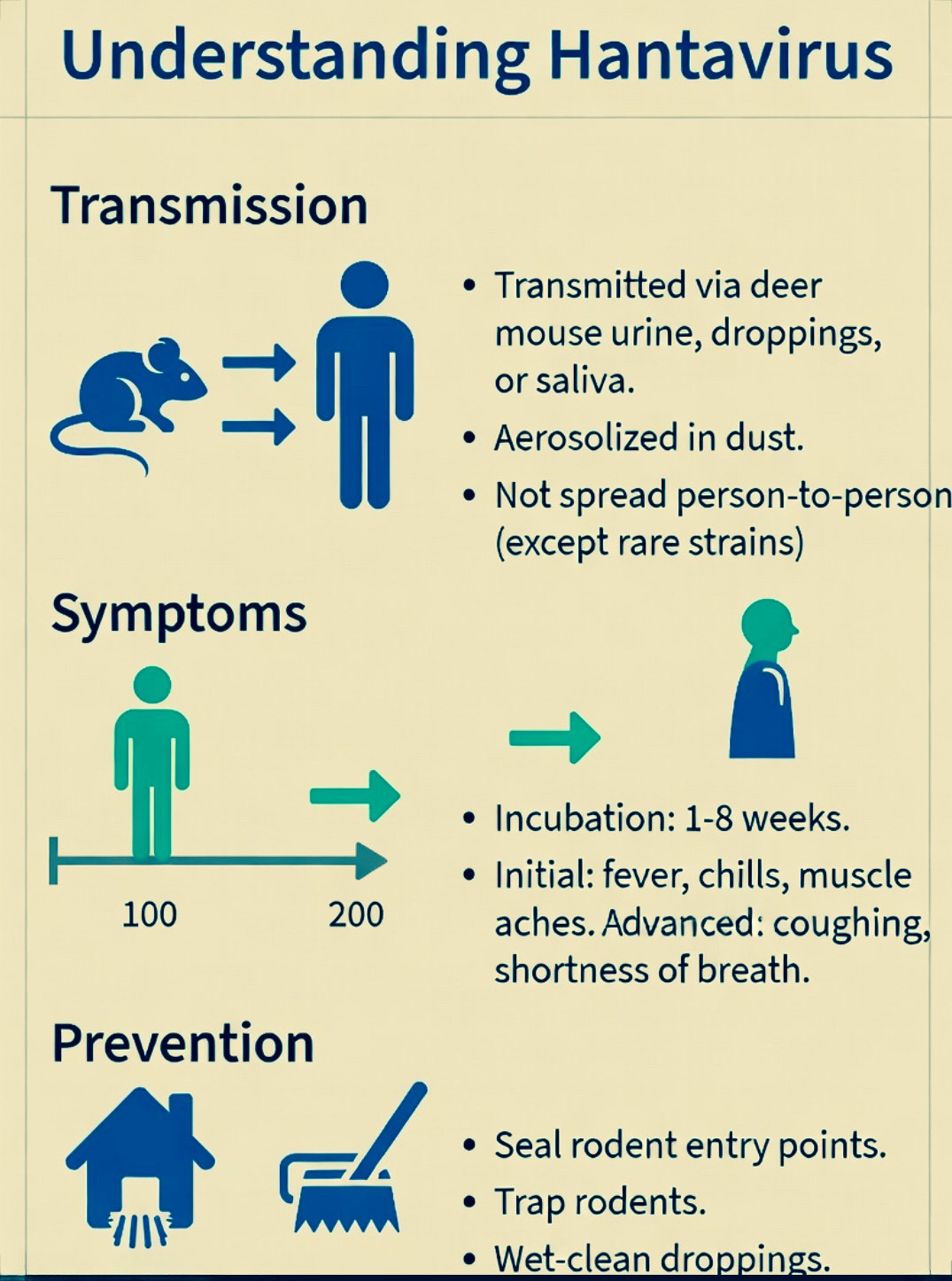
Hantavirus is not new. It has been around and documented in the United States since a mysterious outbreak in the American Southwest in 1993, when a cluster of young, healthy Navajo people died of sudden respiratory failure. Scientists eventually traced it to the deer mouse. Since then, cases have turned up across North and South America, Europe, and Asia, always linked to rodents and almost always involving someone who spent time in places where infected mice or rats had left their droppings, urine, or saliva.
There are more than fifty known types of hantavirus. Most of them spread in exactly one way: you breathe in contaminated dust from rodent droppings, usually in rural cabins, sheds, or fields. You do not catch it from another person. You do not get it at a restaurant or on a subway. It is, in that sense, a virus with a very specific pathway that most people in cities can reasonably not worry about.
The Andes virus is the exception. It is the only known hantavirus documented to spread from person to person, although that spread has typically required close, prolonged contact with someone who is already symptomatic. That distinction is critical to understanding why a cruise ship became a cluster and why health officials worldwide are paying attention.
What happened on the Hondius
The MV Hondius departed Ushuaia, Argentina, the southernmost city in the world, on April 1st, bound for Antarctica and a series of remote South Atlantic islands. It carried roughly 150 passengers and crew representing 23 nationalities. Most passengers came from Spain, France, the United Kingdom, and the United States.
The leading hypothesis from Argentine investigators is that the index case, a Dutch citizen who showed the first symptoms, contracted the virus before boarding. He had completed a four-month road trip through Chile, Uruguay, and Argentina ending just days before the ship departed. He had returned from Uruguay only four days before embarkation.
Once on board, in the close quarters of a ship with shared spaces, recirculated air, and sustained contact between passengers, the virus moved. A passenger died on April 11th. His wife disembarked at Saint Helena and died two days later in a hospital in Johannesburg. A third passenger also died on board. A British passenger was evacuated to South Africa in critical but stable condition.
As of May 8th, the WHO reports eight cases total, six confirmed and two probable, including three deaths, for a case fatality rate of 38 percent. All confirmed cases have been identified as Andes virus through PCR testing. Symptomatic patients are currently hospitalized in South Africa, the Netherlands, Germany, Saint Helena, Spain, and Switzerland.
The CDC has confirmed no cases in the United States as a result of this outbreak and has classified the risk to the American public as extremely low. Routine travel can continue normally. Still, the CDC sent a team to meet the ship in the Canary Islands on May 7th and is coordinating the repatriation of American passengers to a specialized medical facility in Nebraska.
Why the 38 percent number matters
That case fatality rate deserves more explanation, because it is both alarming and contextual.
The WHO reports hantavirus mortality between 1 and 15 percent in Asia and Europe, rising to as high as 50 percent in the Americas. The CDC’s 38 percent figure applies specifically to patients who develop full hantavirus pulmonary syndrome, the severe respiratory form of the disease. Not every infected person reaches that stage. But those who do deteriorate fast.
Symptoms of Andes virus infection typically appear between 4 and 42 days after exposure, beginning with fever, muscle aches, fatigue, and gastrointestinal symptoms before progressing to the lungs. Patients can deteriorate rapidly, and delayed care reduces the chance of survival significantly. In severe cases, a procedure called extracorporeal membrane oxygenation, which takes over the work of the lungs externally, can improve survival to roughly 80 percent if started early.
There is no specific antiviral drug that treats hantavirus. There is no vaccine. Treatment is supportive care: rest, hydration, oxygen, and in severe cases, intubation or ECMO. This is a virus that medicine currently manages rather than defeats.
What makes this outbreak unusual
The hantavirus cases that occur every year in the United States, roughly 30 to 40 annually, almost all involve rural exposure to rodents. Someone cleans out a cabin that has been closed all winter. A farmer works in a grain storage area. A hiker encounters a nest. Those cases are tragic but contained. They do not move between people.
What is happening on the Hondius is different, and scientists are watching it carefully for that reason. The spread on board has been at least partially attributed to human-to-human transmission, given the epidemiological links between cases and the timing of symptom onset clustering around documented incubation periods for the Andes virus.  This is not a rodent problem on a cruise ship. This is the rare strain that can move through sustained human contact, moving through sustained human contact on a vessel where people ate together, shared corridors, and breathed the same recirculated air for weeks.
That does not make it COVID. The Andes virus requires close, prolonged contact with a symptomatic person, not a brief encounter in a hallway. But it makes this outbreak scientifically significant in a way that routine hantavirus cases are not.
What the authorities are saying
The WHO assessed the global risk from this event as low as of May 4th and has not changed that assessment.  The organization notes that the total number of cases remains small, that the virus requires specific conditions to spread between people, and that contact tracing has been aggressive and largely successful. The 30 passengers who disembarked at Saint Helena have all been traced by the UK Health Security Agency.
The CDC’s message to Americans is measured and specific. If you were not on the Hondius, your risk is essentially zero. If you were on the Hondius or had close contact with someone who was, monitor for symptoms and seek medical care immediately if fever, muscle aches, or breathing difficulty develop within 42 days of potential exposure.
For healthcare workers treating potential cases, the CDC recommends airborne infection isolation rooms and full protective gear including N95 respirators.  That guidance reflects appropriate caution rather than evidence of widespread airborne spread.
What we do not know yet
Several important questions remain open. Argentine authorities are still capturing and testing rodents along the route the index patient traveled, trying to pinpoint exactly where and when he was exposed. Genomic sequencing of the virus samples is ongoing, which could clarify the transmission chain more precisely. The full passenger manifests of everyone who disembarked at various ports are still being cross-referenced against reported symptoms globally.
There is also the question of what the ship’s conditions contributed. Recirculated air systems, shared dining spaces, small cabins. Whether ventilation played a role in facilitating transmission aboard the Hondius is something epidemiologists are actively investigating.
What you should actually do
If you live in the United States and have no connection to the Hondius, you do not need to do anything differently today. Hantavirus in America remains an occupational and environmental risk tied to rodent exposure in specific settings, not a community-spread disease.
If you are planning travel to South America, particularly to rural or outdoor areas in Argentina, Chile, or Patagonia, the guidance that has always existed still applies. Avoid contact with rodents and their droppings. Do not sleep in enclosed spaces that show signs of rodent activity without cleaning them thoroughly first. If you develop flu-like symptoms with significant muscle aches after potential exposure, tell your doctor specifically about that exposure. Hantavirus is easy to miss in early stages because it looks like the flu, and timing matters enormously.
The bottom line
Three people are dead. Eight are confirmed or probable cases across six countries. A cruise ship full of passengers from four continents is docking in the Canary Islands right now while health authorities in a dozen countries track everyone who breathed the same air for the past five weeks.
This is not the next pandemic. The WHO and the CDC have been consistent on that. But it is a genuine and ongoing outbreak of one of the deadliest respiratory viruses known to science, spreading through a mechanism that most experts had hoped would remain theoretical. It deserves attention, honest reporting, and the kind of clear-eyed monitoring that early outbreaks always require.
We will keep watching it.
That’s what this letter is for.
— US Daily Letter | May 10, 2026